A53.9
Syphilis serology
The Rapid Plasmin Reagin (RPR) measures disease activity, but is not specific for syphilis. False RPR positive reactions may occur, notably in patients with connective tissue disorders (false positive reactions are usually low titre < 1:8). For this reason, positive RPR results should be confirmed as due to syphilis by further testing of the serum with a specific treponemal test, e.g.:
- Treponema pallidum haemagglutination (TPHA) assay.
- Treponema pallidum particle agglutination (TPPA) assay.
- Fluorescent Treponemal Antibody (FTA) assay.
- Treponema pallidum ELISA.
- Rapid treponemal antibody test. (TPAb)
Screening can also be done the other way around starting with a specific treponemal test followed by a RPR in patients who have a positive specific treponemal test. This is sometimes referred to as the “reverse algorithm”.
- Once positive, specific treponemal tests generally remain positive for life and therefore the presence of specific treponemal antibodies cannot differentiate between current and past infections
- A person with previously successfully treated syphilis will retain lifelong positive specific treponemal test results.
The RPR can be used:
- To determine if the patient’s syphilis disease is active or not,
- To measure a successful response to therapy (at least a fourfold reduction in titre, e.g. 1:256 improving to 1:64), or
- To determine a new re-infection.
Some patients, even with successful treatment for syphilis, may retain life-long positive RPR results at low titres (≤1:8), which do not change by more than one dilution difference (up or down) over time (so-called serofast patients).
Note:
- Up to 30% of early syphilis cases, i.e. those with genital ulcers may have a negative RPR.
- The RPR is always positive in the secondary syphilis stage and remains high during the first two (infectious) years of syphilis.
For syphilis treatment in pregnancy, see Syphilis in pregnancy.
MEDICINE TREATMENT
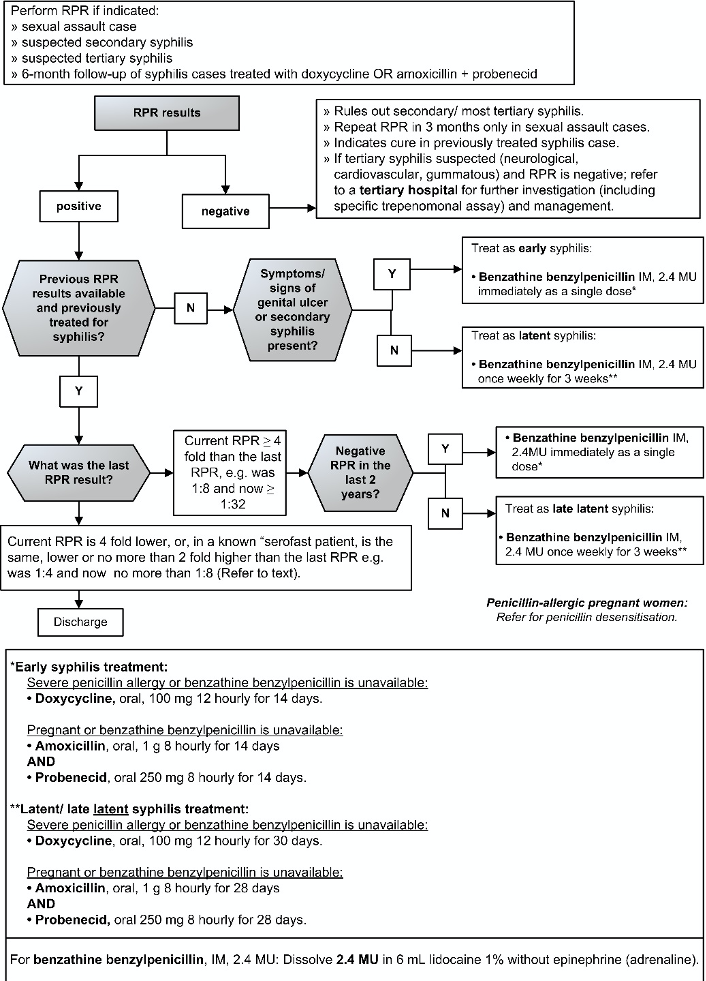
Early syphilis treatment
Check if treated at initial visit.
- Benzathine benzylpenicillin, IM, 2.4 MU immediately as a single dose.
- Dissolve benzathine benzylpenicillin, IM, 2.4 MU in 6 mL lidocaine 1% without adrenaline (epinephrine).
In penicillin-allergic patients or if benzathine benzylpenicillin is unavailable: (Z88.0)
- Doxycycline, oral, 100 mg 12 hourly for 14 days.
If pregnant and benzathine benzylpenicillin is unavailable:
- Amoxicillin, oral 1 g 8 hourly for 14 days (Doctor initiated)
AND
- Probenecid, oral 250 mg, 8 hourly for 14 days (Doctor initiated).
If penicillin-allergic and pregnant: Refer for penicillin desensitisation.
Late/ late latent syphilis treatment
Check if treatment was commenced at initial visit.
- Benzathine benzylpenicillin, IM, 2.4 MU once weekly for 3 weeks.
- Dissolve benzathine benzylpenicillin, IM, 2.4 MU in 6 mL lidocaine 1% without adrenaline (epinephrine)..
In penicillin-allergic patients or if benzathine benzylpenicillin is unavailable: (Z88.0)
- Doxycycline, oral, 100 mg 12 hourly for 30 days.
If pregnant and benzathine benzylpenicillin is unavailable:
- Amoxicillin, oral 1 g 8 hourly for 28 days (Doctor initiated)
AND
- Probenecid, oral 250 mg, 8 hourly for 28 days. (Doctor initiated)
If penicillin-allergic and pregnant: Refer for penicillin desensitisation.
REFERRAL
- Tertiary syphilis: neurosyphilis, cardiovascular syphilis; gummatous syphilis.
- Clinical congenital syphilis.