N95.9
GENERAL MEASURES
Counselling:
- Stop smoking.
- Maintain a balanced diet.
- Regular exercise
MEDICINE TREATMENT
Hormone therapy (HT)
Not indicated in all postmenopausal women. Women with significant menopausal symptoms and those with osteoporosis risk factors will benefit most.
The benefits of HT need to be weighed against the potential harm (e.g. breast cancer, venous thrombo-embolism).
Long-term follow up studies from the Women’s Health Initiative Randomised Trials have shown that hormone replacement therapy in post-menopausal women was not associated with an increased risk of all-cause, cardiovascular or cancer mortality. However, long-term use of hormone therapy has safety issues and stopping treatment will result in return of menopausal symptoms.
Note: Contraindications to HT:
- Current, past or suspected breast cancer.
- Known or suspected oestrogen-dependent malignant tumours.
- Undiagnosed genital bleeding.
- Untreated endometrial hyperplasia.
- Previous idiopathic or current venous thrombo-embolism.
- Known arterial CHD.
- Active liver disease.
- Porphyria.
- Thrombophilia.
Intact uterus (no hysterectomy)
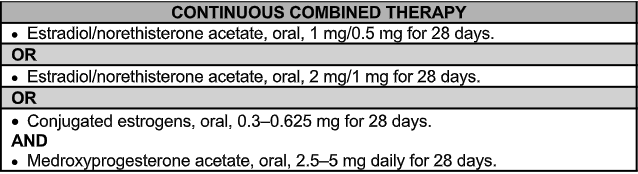
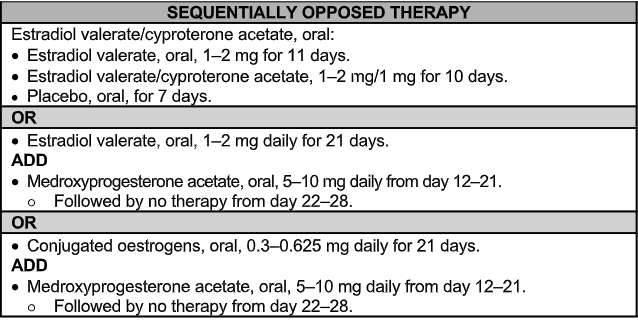
HT can be offered as sequentially opposed or continuous combined preparations. Continuous combined preparations have the advantage of less breakthrough bleeding, but should only be commenced once the woman has been stable on sequentially opposed therapy for a year. Treatment should be planned for 5 years but reviewed annually.
OR
Note:
- Start at the lowest possible dose to alleviate symptoms. The need to continue HT should be reviewed annually. Abnormal vaginal bleeding requires specialist consultation/referral.
- Any unexpected vaginal bleeding is an indication for excluding endometrial carcinoma. The use of transvaginal ultrasound to measure endometrial thickness plus the taking of an endometrial biopsy are recommended.
Uterus absent (post hysterectomy): (Z90.7)
HT is given as estrogen only:
- Estradiol valerate, oral, 1–2 mg daily.
OR
- Conjugated equine estrogens, oral, 0.3 mg daily or 0.625 mg on alternative days up to a maximum of 1.25 mg daily.
HT is contra-indicated, poorly tolerated or ineffective:
- Fluoxetine, oral
- Initiate at 20 mg on alternate days.
- If there is no response after 12 weeks, increase the dose to 20 mg daily.
If on tamoxifen:
- Citalopram, oral, 10 mg daily.
- If there is no response after 12 weeks, increase the dose to 20 mg daily.
Note:
Start at the lowest possible dose to alleviate symptoms. The need to continue therapy should be reviewed annually.
REFERRAL
- Premature menopause, i.e. <40 years of age.
- Severe osteoporosis.
- Post-menopausal bleeding.
- Hormone-dependent cancers, thrombo-embolism, liver disease; and unacceptable side-effects to hormone replacement therapy e.g. exacerbation of depression, enlargement of uterine fibroids, exacerbation of endometrioses (see Endometriosis).