Patients on anticoagulants are at risk of developing a spinal haematoma with subsequent paralysis after a spinal or epidural block. These anticoagulants should be stopped before the spinal or epidural is performed according to the guidelines given below. In order to encourage safe and quality care of patients, please consult a specialist prior to attempting blocks on patients on anticoagulants. There are a range of oral anticoagulation, with each having specific recommendations with regard to neuraxial blocks.
Timing of anticoagulants in patients receiving neuraxial anaesthesia:
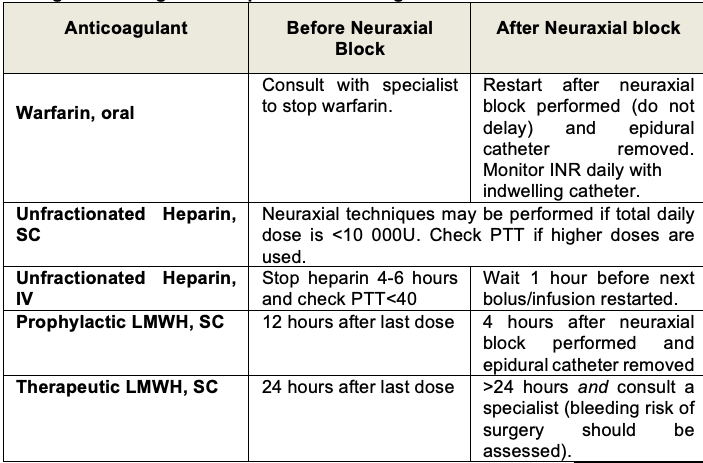
Note. After neuraxial block or epidural catheter removal, patients should be observed closely for new or progressive neurological symptoms. A spinal haematoma can result in permanent paralysis unless decompressive surgery is performed within 8 hours of paralysis onset.
Clopidogrel and platelet GPIIb/IIIa inhibitors have variable durations of effects on clotting after stopping these medications. Specialist advice should be sought before performing neuraxial blocks on patients receiving these medications.
For patients on warfarin the use of bridging anticoagulation (giving heparin after warfarin is stopped in preparation for surgery or invasive procedures) remains unsettled. Practitioners should exercise careful judgment of competing risks in individual patients. Heparin may increase the risk of bleeding. Whatever practice is adopted the most important consideration is to ensure that adequate anticoagulation with warfarin is re-instituted once the risk of bleeding is past.